MD Review of Somatic Tinnitus
Many of my patients want to know more about somatic tinnitus. Interestingly, somatic tinnitus has several powerful links to migraine and may itself be a form of atypical migraine. Here, I’ll cover these topics:
- What is somatic tinnitus?
- What is the relationship between migraine and somatic tinnitus?
- Is somatic tinnitus really atypical migraine in disguise?
- How do you treat somatic tinnitus?
- What is the best treatment for somatic tinnitus?
What is somatic tinnitus?

Somatic tinnitus refers to cases when tinnitus is modulated by ‘somatic’ factors, meaning factors related to the body’s sensory system and physical sensations. Most commonly, it’s seen in patients with co-existing jaw or neck pain, where these symptoms are thought to contribute to or worsen tinnitus symptoms.
What are somatic tinnitus symptoms?
In somatic tinnitus, various somatosensory factors can influence the perception of tinnitus, including:
- Neck or jaw pain that occurs simultaneously with tinnitus.
- Symptoms in the neck or jaw that worsen tinnitus symptoms.
- Head or neck surgery that precedes the onset of tinnitus.
- Variability in the pitch, loudness, and/or location of the perceived sound.
- Discrepancies between the hearing test and the characteristics of tinnitus.
Somatic tinnitus patients find that certain movements or manipulations of the head, neck, jaw, or eyes can modulate their tinnitus. Additionally, somatic maneuvers and the application of pressure on myofascial trigger points may also impact the perception of tinnitus.
‘Somatosensory tinnitus’ and ‘somatic tinnitus’ are essentially interchangeable terms, both referring to the phenomenon where bodily sensations influence the perception of tinnitus.

How common is somatosensory tinnitus?
As a tinnitus specialist, the majority of my patients show signs and symptoms consistent with somatic tinnitus. A recent study found that the average prevalence of somatosensory modulation of tinnitus across multiple studies is 69% [1]. This may be more prevalent in certain subgroups of individuals, such as those with temporomandibular joint disorders (TMDs), cervical spine dysfunction, or a history of head and neck surgery.
Likewise, tinnitus patients are much more likely to have somatic conditions of the head and neck region. A recent study found patients with chronic subjective tinnitus were 6.7x more likely to have TMDs and 2.6x more likely to have cervical spine dysfunction than patients without tinnitus [2].
What are the clinical features of somatic tinnitus?
The clinical presentation can vary widely among individuals, but there are several common characteristics and features seen in somatosensory tinnitus:
| Characteristic | Description |
|---|---|
| Presence of Tinnitus | Somatic tinnitus is often described as ringing, buzzing, humming, pulsating, or clicking noises that correlates with somatic factors. |
| Modulation by Somatic Factors | The tinnitus perception is influenced by changes in body conditions, such as head or neck movements, jaw clenching, changes in posture, or muscle tension. |
| Musculoskeletal Issues | People with somatic tinnitus may have concurrent musculoskeletal issues, such as temporomandibular joint (TMJ) disorders, cervical spine issues, or muscle tension in the head, neck, and shoulder regions. |
| Fluctuating Nature | Tinnitus symptoms in somatic tinnitus tend to be fluctuating in nature, where the tinnitus and somatic symptoms are coincident. |
| Comorbidities | Somatic tinnitus is frequently associated with migraine, anxiety, depression, and sleep disturbances. |
| Quality of Life | Somatic tinnitus can have a significant impact on quality of life, leading to distress, anxiety, difficulty concentrating, sleep disturbances, and impaired social and occupational functioning. |
| Somatic Manipulation | Some people with somatic tinnitus find relief or modulation of their symptoms through somatic manipulation techniques, such as jaw exercises, physical therapy, or relaxation techniques. |
How do you diagnose somatic tinnitus?
Diagnosing somatic tinnitus involves a comprehensive evaluation, including:
- Medical History: Assessing tinnitus history for somatic symptoms.
- Physical Examination: Evaluating the head, neck, and jaw for signs of dysfunction.
- Audiological Assessment: Testing hearing function to rule out hearing pathology.
- Imaging Studies: Using scans to identify structural abnormalities or vascular issues.
- Specialized Assessments: Employing tests to evaluate TMJ function.
- Collaboration: Working with other healthcare providers for multidisciplinary treatment planning.
By conducting a thorough evaluation, clinicians can identify underlying somatosensory dysfunctions and tailor treatment strategies for somatosensory tinnitus patients.
What are somatic maneuvers?
Somatic maneuvers encompass a range of specific movements or actions aimed at assessing their impact on tinnitus perception, particularly in relation to the jaw and neck regions. Here are some examples of jaw and neck maneuvers commonly used in clinical practice:
| Somatic Maneuver | Description |
|---|---|
| Teeth Clenching | Patients clench their teeth together firmly, assessing any changes in tinnitus perception during and after the clenching motion. |
| Mouth Opening | Patients open their mouth as wide as possible, noting any modulation of tinnitus symptoms during the opening motion. |
| Jaw Protrusion | Patients move their jaw forward to assess its effect on tinnitus perception (with or without applied pressure). |
| Lateral Jaw Movement | Patients move their jaw side-to-side to evaluate its influence on tinnitus symptoms (with or without applied pressure). |
| Resistance to Force | Keeping the patient’s head in a neutral position, the patient notes any changes in tinnitus perception when pressure is applied in different directions against resistance. |
| Head Movements | Various head movements (forward, backward, lateral bending, and rotation) are performed while observing for any modulation of tinnitus symptoms during each movement. |
| Torsional Force Exertion | The patient’s head is turned to one side and slight torsional force is applied to the cheekbone on the same side to check for tinnitus worsening. |
By systematically evaluating the influence of these maneuvers on tinnitus perception, we can better understand the underlying mechanisms contributing to somatosensory tinnitus and tailor treatment strategies accordingly.
Is there a relationship between somatic tinnitus and unilateral tinnitus?
There does appear to be is a relationship between unilateral tinnitus and somatic tinnitus, particularly in the context of temporomandibular joint (TMJ) disorders. Research indicates that people with unilateral tinnitus may experience somatic modulation of their symptoms, especially in regions associated with the affected side.
Can somatic tinnitus affect pulsatile tinnitus?
While somatosensory tinnitus and pulsatile tinnitus are distinct, they can coexist in some individuals. For example, somatic factors such as changes in muscle tension or jaw position may exacerbate pulsatile tinnitus or influence its perception. Pulsatile tinnitus is an objective tinnitus subtype, meaning that it’s cause is vascular, not neurological.
What is the relationship between migraine and somatic tinnitus?

Migraine and somatic tinnitus share a complex relationship that involves overlapping neural pathways and sensory processing mechanisms, particularly within the trigeminal system and the trigeminocervical complex. These lend evidence to the fact that somatic tinnitus may be related to an underlying migraine-like process.
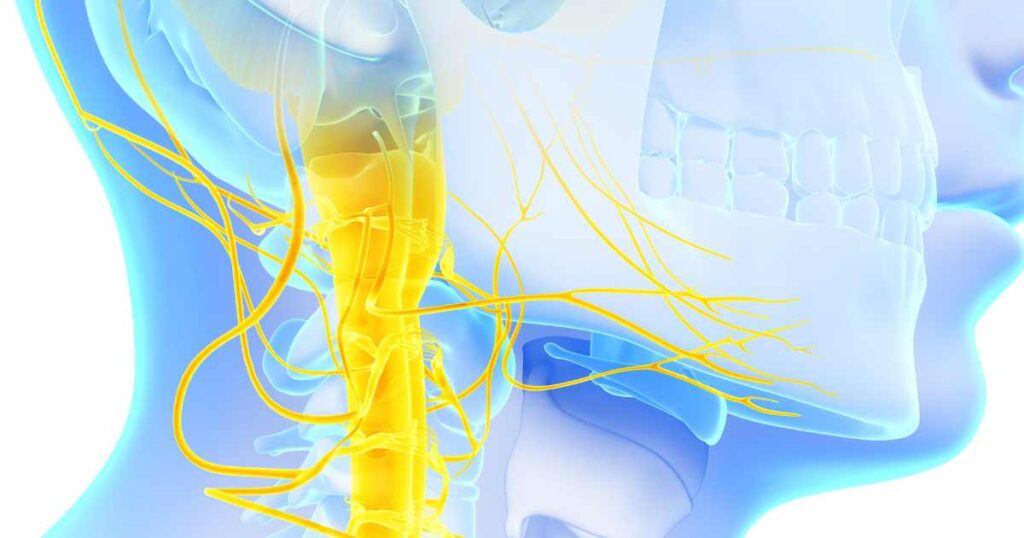
What is the role of the trigeminal nerve in somatic tinnitus?
The trigeminal nerve, also known as the fifth cranial nerve (CN5), plays a significant role in somatic tinnitus due to its extensive innervation of the head and face. It is also the primary nerve involved in the migraine process. The trigeminal nerve transmits sensory information from various parts of the head, including the temporomandibular joint (TMJ), muscles of mastication, teeth, gums, parts of the neck, and the ear region.
In cases of somatosensory tinnitus, dysfunction or irritation of the trigeminal nerve can contribute to the perception of tinnitus. This can occur due to several reasons:
| Clinical Context | Trigeminal Nerve Connection |
|---|---|
| Temporomandibular Joint Disorders | The TMJ is innervated by the trigeminal nerve and is commonly associated with somatic tinnitus. TMJ conditions can lead to referred pain and sensory disturbances that may influence tinnitus intensity. |
| Dental Problems | Dental issues such as bruxism (teeth grinding), malocclusion (misalignment of teeth), or dental trauma can affect the trigeminal nerve and contribute to somatic tinnitus. |
| Muscular Tension | Muscular tension in the head, neck, and shoulder region can exacerbate somatic tinnitus via trigeminal connections. Chronic tension in these muscles may alter sensory inputs and influence tinnitus perception. |
| Neuropathic Pain Syndromes | Conditions such as trigeminal neuralgia may also be associated with somatic tinnitus. The aberrant firing of trigeminal nerve fibers can impact sensory processing and contribute to tinnitus intensity. |
| Neck-Jaw Integration | The trigeminal nerve interacts with the auditory system at various levels, leading to somatosensory-auditory interactions that can modulate tinnitus perception. |
How can neck problems cause tinnitus?
The trigeminocervical complex (TCC), situated within the brainstem, serves as a critical nexus for sensory processing, where inputs from the trigeminal nerve and upper cervical nerves converge and interact. This convergence is particularly relevant in understanding somatic tinnitus, as it sheds light on how neck and jaw pain can be intricately linked to both migraine and tinnitus.
In cases of somatosensory tinnitus, sensitization of the TCC due to conditions such as temporomandibular joint (TMJ) disorders or cervical spine issues can contribute to the perception of tinnitus. The TCC integrates sensory information from the trigeminal nerve, which innervates the face and jaw, and the upper cervical nerves, which innervate the neck and back of the head. Dysfunction in these areas can lead to aberrant sensory processing and modulate tinnitus perception.
Furthermore, the TCC’s involvement in migraine pathophysiology underscores the interconnectedness of neck and jaw pain with both migraine and tinnitus. Migraine is known to involve dysfunction of the trigeminovascular system, where nociceptive signals from cranial blood vessels converge with inputs from the trigeminal nerve within the TCC, leading to headache and associated symptoms. Neck and jaw pain commonly accompany migraine attacks, reflecting the convergence of sensory inputs from these regions within the TCC.
CGRP and Somatic Tinnitus
One key player in this relationship is the calcitonin gene-related peptide (CGRP), a neuropeptide involved in pain transmission and modulation. CGRP is implicated in the pathophysiology of both migraine and somatic tinnitus.
In migraine, CGRP plays a crucial role in vasodilation and neurogenic inflammation within the trigeminal system, contributing to headache pain, jaw and neck pain, and tinnitus. Similarly, in somatic tinnitus, dysregulation of CGRP signaling within the trigeminal ganglion and other sensory pathways may influence severe tinnitus, potentially exacerbating symptoms through mechanisms such as central sensitization. In other words, somatic tinnitus and atypical migraine are identical from a neurobiology point of view.
The Trigeminal Ganglion and Somatic Tinnitus
The trigeminal ganglion, which houses the cell bodies of sensory neurons innervating the head and face, is another site of convergence for migraine and somatosensory tinnitus. Dysfunction or sensitization of trigeminal ganglion neurons can lead to aberrant sensory processing and the generation of pain signals characteristic of migraine. Moreover, the trigeminal ganglion is implicated in somatosensory-auditory interactions, providing another link between trigeminal dysfunction and the modulation of subjective tinnitus.
Implications for Somatic Tinnitus Treatment
It’s clear that migraine and somatic tinnitus involves shared neural pathways at multiple levels. Understanding these shared mechanisms, such as CGRP signaling and sensory processing within the TCC, is crucial for understanding the interplay between migraine and somatic tinnitus and developing targeted therapeutic interventions for both conditions.
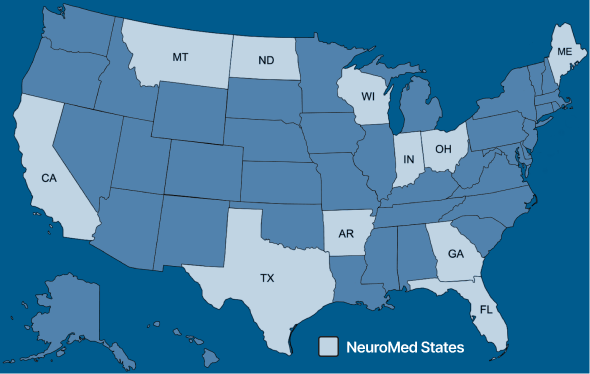
In practice, multiple studies have shown that somatic tinnitus responds exceptionally well to migraine treatments. In fact, nearly all patients with somatic tinnitus show dramatic improvement using protocols at NeuroMed, which are geared towards treating the migraine reaction in the brain.
Is somatic tinnitus really atypical migraine in disguise?

Somatic tinnitus shares several key characteristics and associations with migraine. Here’s a summary of why somatic tinnitus should be considered a variant or manifestation of atypical migraine:
| Feature | Description |
|---|---|
| Overlap in Clinical Features | Somatic tinnitus and migraine often share common clinical features, including headache, neck pain, jaw discomfort, and sensory disturbances. This suggests a shared underlying pathophysiology. |
| Trigeminal Involvement | Both somatic tinnitus and migraine involve dysfunction of the trigeminal system, a key mediator of pain and sensory processing in the head and face. Both are associated with trigeminal activation and neurogenic inflammation. |
| Comorbidities and Associations | Somatic tinnitus and migraine frequently co-occur with anxiety, depression, and sleep disturbances. Additionally, both are associated with musculoskeletal issues, such as TMDs and cervical spine dysfunction. |
| Fluctuating Nature | Both somatic tinnitus and migraine are characterized by fluctuating symptoms. These fluctuations can often be traced to shared environmental triggers, including stress, sensory overstimulation, and certain food items. |
| Response to Treatment | People with somatic tinnitus respond to migraine treatments, such as stress reduction techniques, regular exercise, and dietary changes, suggesting shared mechanisms and treatment targets between the two conditions. |
| Neurological Basis | Both somatic tinnitus and migraine involve complex neurobiological processes, including central sensitization, cortical hyperexcitability, and altered sensory processing, providing further evidence of a shared mechanism. |
In conclusion, the similarities in clinical features, trigeminal involvement, comorbidities, treatment response, and underlying neurobiology suggest that somatic tinnitus is a variant or manifestation of atypical migraine.
How do you treat somatic tinnitus?

Treatment for somatic tinnitus is a multifaceted process that involves addressing underlying somatosensory dysfunctions contributing to the perception of tinnitus. This comprehensive approach integrates various strategies tailored to the individual patient’s needs.
Typically, addressing only the body part involved as a monotherapy yields mediocre results. For the best care, an integrated strategy should be used.
Does physical therapy help with somatic tinnitus?
Physical therapy techniques are commonly employed to alleviate somatosensory tinnitus symptoms by targeting musculoskeletal dysfunctions, such as temporomandibular joint (TMJ) disorders or cervical spine issues. However, results are fairly poor when used as the sole intervention for somatic tinnitus.
Jaw exercises, manual therapy, and techniques to improve posture and muscle tension are common interventions. Additionally, trigger point release, myofascial release, and stretching exercises may be utilized to address muscular tension and pain in the head, neck, and shoulder regions. Furthermore, biofeedback, relaxation techniques, and acupuncture can play a role in managing stress and tension in the neck and jaw.
The clinical data is poor in most studies as they fail to report effect sizes and do not include appropriate control groups. In fact, it’s unclear if these physical medicine interventions have any effect greater than standard tinnitus treatments. For instance, one study found that somatic tinnitus patients respond excellently to the kind of modified Tinnitus Retraining Therapy we offer at NeuroMed (i.e. using education alone without formal physical therapy) [3].
Does neck surgery help somatic tinnitus?
In cases where somatic tinnitus patients is attributed to structural abnormalities or pathologies in the cervical spine, surgical intervention may be considered. Surgical procedures such as cervical spine fusion, decompression surgery, or disc replacement may be recommended to address cervical spine issues contributing to tinnitus symptoms.
However, surgical intervention is typically reserved for cases where conservative treatments have failed to provide relief, where there is radiological confirmation of significant cervical disease, and the benefits outweigh the risks. Unfortunately, I’ve seen several patients who underwent unnecessary neck surgery in a failed attempt to address somatosensory tinnitus symptoms.
What is the Susan Shore Device?
The Susan Shore Device (SSD) is a form of bimodal stimulation for tinnitus, meaning that it combines sound therapy with a secondary form of sensory stimulus. In the case of the SSD, the secondary form of stimulation is through electrical signals to the jaw or neck region. Many are hoping that the device will prove particularly useful for people with somatic tinnitus, given the secondary region of stimulation. It is not currently FDA approved or available for commercial use.
The problem with the SSD (and with other bimodal devices like Lenire) is that it only addresses the sound therapy and habituation portion of tinnitus recovery and ignores the contribution of the migraine process. Further, all pilot studies published to date on the SSD (or similar devices) show that they fail to show any more improvement than front-line interventions like tinnitus CBT and sound therapy.
Does migraine treatment help somatic tinnitus?
Migraine management strategies are integral in reducing somatosensory tinnitus symptoms. Medications commonly used to prevent or alleviate migraine attacks help reduce somatic tinnitus patients. Further, lifestyle modifications, including stress management, regular exercise, adequate sleep, and dietary changes, can complement pharmacological treatments and contribute to tinnitus symptom relief. Botox injections, approved for the treatment of chronic migraine, may provide relief for somatic tinnitus symptoms by reducing muscle tension and pain in the head and neck region.
What is the best treatment for somatic tinnitus?

We have found excellent results using our integrative medicine protocols to lower tinnitus severity in patients with somatosensory tinnitus. Our protocols are based on the knowledge that tinnitus loudness is fundamentally related to a migraine-like process in the brain. This may be especially true of somatic tinnitus patients given the strong association between this tinnitus subtype and migraine.
Elements of our tinnitus management protocol include:
- Pharmaceutical Therapy
- Nutraceutical Therapy
- Cognitive Behavioral Therapy
- Sound Therapy
- Mindfulness Meditation
- Dietary Therapy
- Sleep Optimization
- Physical Exercise
In addition, for patients where somatosensory nerves may be contributing to the patient’s tinnitus, we advocate for parallel use of physical therapy treatments to reduce tinnitus, including manual therapy, massage, jaw and neck exercises, acupuncture, and Botox treatment.
Conclusion: Somatic Tinnitus Is Treatable!
Somatosensory tinnitus, characterized by the modulation of tinnitus symptoms by somatic factors, presents a unique challenge in diagnosis and management. Understanding the complex interplay between sensory systems, musculoskeletal function, and neurological pathways is crucial for effectively treating tinnitus.
Here, we’ve explored the relationship between somatic tinnitus and migraine, highlighting shared mechanisms and treatment strategies. In fact, from my point of view as a tinnitus specialist, I’m confident that somatosensory tinnitus is more accurately characterized as an atypical migraine variant.
By addressing underlying somatosensory dysfunctions and incorporating multidisciplinary approaches, including physical therapy, migraine treatment, and lifestyle modifications, significant improvements in tinnitus severity and quality of life can be achieved. Somatosensory tinnitus is a treatable condition, and with comprehensive tinnitus management, patients can experience meaningful relief from their symptoms.
Somatosensory Tinnitus References
[1] Ralli M, Greco A, Turchetta R, Altissimi G, de Vincentiis M, Cianfrone G. Somatosensory tinnitus: Current evidence and future perspectives. J Int Med Res. 2017 Jun;45(3):933-947.
[2] Bousema EJ, Koops EA, van Dijk P, Dijkstra PU. Association Between Subjective Tinnitus and Cervical Spine or Temporomandibular Disorders: A Systematic Review. Trends Hear. 2018 Jan-Dec;22:2331216518800640.
[3] Ostermann K, Lurquin P, Horoi M, Cotton P, Hervé V, Thill MP. Somatic tinnitus prevalence and treatment with tinnitus retraining therapy. B-ENT. 2016;12(1):59-65.